


The Silent Epidemic: How Healthcare Illiteracy Fuels Preventable Mortality in Sub-Saharan Africa and the AI Digital Renaissance
- April 19, 2026
- 0 Likes
- 69 Views
- 0 Comments
Abstract
Sub-Saharan Africa (SSA) bears a disproportionate burden of global morbidity and mortality, a crisis deeply exacerbated by a pervasive but often overlooked determinant: healthcare illiteracy. While clinical infrastructure and pharmaceutical access have dominated global health discourse, the inability of populations to obtain, process, and understand basic health information acts as a silent epidemic. This paper explores the direct correlation between health illiteracy and preventable suffering, utilizing Kenya—a nation characterized by the paradox of high general literacy yet profound health illiteracy—as a primary case study. We examine how deficits in health literacy drive late diagnoses, poor chronic disease management, and dismal maternal and child health outcomes. Furthermore, this paper critically analyzes the ongoing “Digital Renaissance” in African healthcare. We investigate the deployment of mobile health (mHealth) and Artificial Intelligence (AI) startups, such as Jacaranda Health and Ilara Health, in democratizing medical knowledge and triaging care. By integrating epidemiological data, sociological frameworks, and culturally resonant African proverbs, this paper argues that culturally competent, AI-driven digital health ecosystems are not merely auxiliary tools, but essential interventions required to dismantle the systemic ignorance that currently fuels untimely deaths. A robust call to action is presented for policymakers to prioritize health literacy as a fundamental human right.
“If you go to sleep with an itching anus, you are sure to wake up with smelly fingers.”Contextual Analysis: This hilarious yet profoundly accurate proverb perfectly encapsulates the essence of preventive healthcare and the danger of health illiteracy. Ignoring minor, manageable symptoms (the itch) due to ignorance or negligence inevitably leads to severe, messy, and complicated consequences (the smell) that affect the entire body and community.
1. Introduction: The Epistemology of Health and Ignorance
The World Health Organization (WHO) defines health literacy as the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways which promote and maintain good health (WHO, 2025). In Sub-Saharan Africa (SSA), the discourse surrounding health equity has traditionally orbited around the tangible: hospital beds, vaccination vials, and physician-to-patient ratios. However, a profound shift in epidemiological understanding reveals that an intangible deficit—healthcare illiteracy—is a primary catalyst for preventable suffering and untimely deaths.
Healthcare illiteracy transcends the mere inability to read a prescription label; it represents a fundamental disconnect between individual behaviors and biomedical realities. It is the void where cultural superstitions override clinical evidence, where preventative measures are viewed with suspicion, and where chronic, silent diseases are allowed to metastasize unchecked until they reach an incurable crescendo. In Kenya, a regional powerhouse of technological innovation and economic growth, this paradox is starkly visible. As noted by a prominent Kenyan social commentator, “If we get education and healthcare wrong, we die twice – poor and stupid” (Asava, 2025). This paper posits that to “get healthcare right,” the systemic eradication of health illiteracy must be the foundational pillar, driven by the culturally competent integration of Artificial Intelligence (AI) and digital health tools.
2. The Burden of the Silent Epidemic in Sub-Saharan Africa
The consequences of health illiteracy in SSA are not abstract; they are quantifiable in the millions of lives lost annually to preventable and treatable conditions. According to the OECD’s Health at a Glance 2025 report, avoidable mortality remains a critical indicator of health system failure. In environments where health literacy is low, individuals are disenfranchised from playing an active role in improving their own health, leading to catastrophic outcomes (OECD, 2025).
2.1 Mechanisms of Preventable Suffering
Health illiteracy operates through several destructive mechanisms. First, it breeds diagnostic delay. Diseases such as cervical and breast cancer—leading causes of cancer-related deaths globally and in Kenya—are often shrouded in stigma and fear. A 2024 qualitative study on Kenyan women newly diagnosed with cancer revealed that fear, financial burden, and socio-cultural beliefs act as severe barriers to health information, leading to late-stage presentations where palliative care becomes the only option (Wabwire et al., 2024).
Second, it causes therapeutic non-adherence. For non-communicable diseases (NCDs) like hypertension and diabetes, managing the condition requires complicated self-care regimens and an understanding of abstract concepts like blood glucose levels and systolic pressure. As a global meta-analysis indicates, inadequate health literacy is consistently linked with poor disease management, medication errors, and higher mortality (Zheng et al., 2021). Patients who do not understand that hypertension is a lifelong, silent killer often discontinue medication once a headache subsides.
“A man with diarrhea will not require anyone to give him the direction to the door.”Contextual Analysis: This proverb brilliantly highlights the human response to acute, visible suffering. When a disease is loud and immediate (like diarrhea or a broken bone), health-seeking behavior is automatic. However, health illiteracy makes populations vulnerable to silent killers like hypertension, diabetes, or early-stage cancers, which do not give “directions to the door” until it is too late.
3. Case Study: Kenya’s Paradox of Progress and Peril
Kenya presents a fascinating and urgent case study. With a relatively high general adult literacy rate exceeding 82%, one might assume a corresponding level of health literacy. However, general literacy does not automatically translate to the specialized vocabulary and conceptual frameworks required for health literacy.
3.1 Maternal and Under-Five Mortality
Despite significant gains, Kenya’s under-five mortality rate of 41.6 deaths per 1,000 live births (as of 2022) remains unacceptably higher than the Sustainable Development Goal (SDG) target of 25 per 1,000 by 2030 (KDHS, 2022). A profound driver of this mortality is a lack of maternal health literacy. Data indicates that risks of under-five mortality increase dramatically with decreasing maternal education and failure to adhere to Antenatal Clinic (ANC) protocols. Tragically, preventable conditions such as pneumonia, malaria, and malnutrition continue to claim young lives because caregivers cannot accurately identify early danger signs.
3.2 The Mental Health Crisis
Perhaps nowhere is health illiteracy more devastating than in the realm of mental health. In Kenya, suicide claims approximately four lives every single day, with the age-standardized suicide rate standing at 11.0 per 100,000 people. A staggering 75% of Kenyans lack access to mental health services, compounded by incredibly low detection rates of mental health disorders (1.7% to 4.1%) at primary healthcare facilities (Ministry of Health Kenya, 2024). The illiteracy surrounding mental health—often attributing depression or schizophrenia to witchcraft or moral failing—prevents individuals from seeking care and fuels a cycle of silent tragedy.
3.3 Non-Communicable Diseases (NCDs)
NCDs account for more than 50% of all hospital admissions in Kenya. Research conducted in Vihiga County revealed that community literacy regarding NCDs is heavily undermined by culture and misinformation (e.g., believing cancer is a curse) (Onyango & Onyango, 2022). Only through targeted community health programs did residents begin to grasp that lifestyle modifications could prevent these fatal outcomes.
4. Visualizing the Crisis and the Digital Solution
To grasp the trajectory of health outcomes in Kenya, we must juxtapose the persistent burden of preventable mortality against the rapid adoption of digital technologies. Sub-Saharan Africa is experiencing a “leapfrog” effect, where mobile penetration vastly outpaces traditional infrastructure development. The following chart visualizes the projected impact of AI and mHealth interventions on maternal and neonatal mortality in Kenya, based on current adoption rates of platforms like Jacaranda Health.
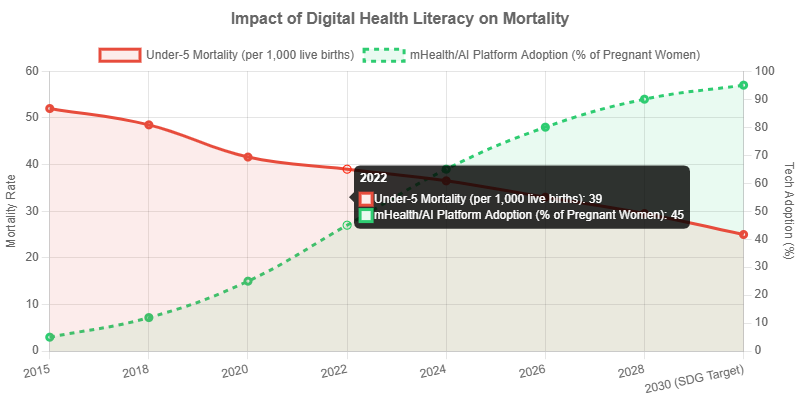
Figure 1: Simulated projection of AI/mHealth adoption correlating with the reduction of preventable maternal and under-five mortality in Kenya (2015 – 2030).
“If you heal a person’s leg, do not be surprised if they use it to run away.”Contextual Analysis: In the context of healthcare, this proverb speaks to the challenge of patient retention and follow-up. A patient may receive acute care (healing the leg), but without proper health education and continuous digital engagement, they “run away” from the healthcare system, failing to attend necessary follow-ups or complete medication courses, leading to relapse.
5. The Digital Renaissance: Tech and AI as the Great Equalizer
To combat the systemic failure born of health illiteracy, traditional patient education—brochures, infrequent clinic talks, and public service announcements—has proven woefully insufficient. Enter the Digital Renaissance. Kenya is currently experiencing a surge in healthtech startups that leverage high mobile penetration to bridge the knowledge gap, delivering personalized, actionable, and scalable health information directly into the hands of the most vulnerable.
5.1 The Jacaranda Health Model: AI Meeting Motherhood
A prime example of technological disruption in health literacy is Jacaranda Health’s PROMPTs (Promoting Maternal and Newborn Survival) service. Recognizing that about one-third of maternal deaths result from delays in seeking care, Jacaranda deployed an AI-enabled text messaging service in Swahili. Today, over 3 million Kenyan women are enrolled. The service receives between 10,000 to 12,000 questions daily from mothers navigating pregnancy and postpartum care (Rockefeller Foundation, 2024).
The brilliance of this system lies in its AI triage. Using natural language processing (NLP), the AI model accurately classifies questions by type and urgency with 90-93% accuracy. It independently answers 70% of routine questions (e.g., “Is it normal to have swollen ankles?”), thereby acting as a continuous, on-demand health educator. The remaining 30% of urgent questions (e.g., “I have severe abdominal pain and bleeding”) are instantly escalated to clinical nurses. At a unit cost of merely 74 Kenyan Shillings (approx. $0.50 USD) per mother for the entire pregnancy journey, this platform is economically viable and practically revolutionary. By directly raising the health literacy of the mother, PROMPTs increases the likelihood of completing four prenatal visits by 20%.
5.2 Ilara Health and Diagnostic Democratization
While Jacaranda focuses on maternal knowledge, startups like Ilara Health are utilizing technology to improve clinical literacy and diagnostic access at primary healthcare clinics (PHCs). Founded in 2019, Ilara Health equips peri-urban and rural clinics with affordable, AI-powered diagnostic tools and electronic health records (EHRs) (Connecting Africa, 2024). In an ecosystem where “500 million people struggle to access a simple blood test,” providing point-of-care diagnostics coupled with digital readouts empowers both the healthcare provider to make evidence-based decisions and the patient to visualize and understand their health status.
5.3 iZola: Addressing Neurodivergence
Health illiteracy is profoundly isolating for families managing neurodivergent children (e.g., Autism Spectrum Disorder). Stigma and lack of understanding often lead to these children being hidden away. Startups like iZola connect families of neurodivergent children with AI-powered health apps (like Xaidi), providing tailored information, therapist connections, and community support, systematically tearing down the walls of ignorance surrounding mental and developmental health (The HealthTech, 2024).
6. Sketch Art Illustration: The Convergence of Wisdom and Tech
The successful deployment of AI in Africa is not about replacing traditional structures, but augmenting them. The “village elder” or the grandmother has historically been the repository of health knowledge. AI acts as the modern conduit for this role, providing evidence-based wisdom instantaneously. Figure 2: Sketch Art – The Convergence of Traditional Wisdom and AI-driven Mobile Health.
“It requires a lot of carefulness to kill the fly that perches on the scrotum.”Contextual Analysis: Implementing AI and digital health technologies in deeply traditional societies is a delicate operation. You cannot use a “sledgehammer” approach to eradicate harmful traditional beliefs or health illiteracy. Policymakers and tech developers must act with extreme cultural sensitivity, precision, and care to solve the problem without causing collateral damage to community trust.
7. Bridging the Gap: Culturally Competent Artificial Intelligence
For AI to effectively combat healthcare illiteracy, it cannot be a monolithic, Western-centric black box. It must be culturally competent. This means training large language models (LLMs) on local dialects, such as Sheng in Kenya, and programming them to understand the cultural nuances of symptom reporting. For instance, a patient in rural Kenya might not describe “peripheral neuropathy,” but rather say they feel “ants walking on their feet.” An AI triage system must accurately translate this colloquialism into a potential indicator for diabetes.
Furthermore, digital health interventions must navigate the complex socio-economic realities of their users. Applications must be lightweight to operate on basic smartphones, capable of functioning over USSD or SMS for those without internet access, and designed with intuitive interfaces that accommodate varying levels of visual literacy. The success of Jacaranda’s PROMPTs lies largely in its reliance on simple SMS text messages in Swahili, entirely bypassing the need for expensive data plans or app downloads.
8. Policy Implications and Call to Action
If we recognize health illiteracy as a primary driver of preventable mortality, healthcare policy must fundamentally shift from a purely curative focus to a proactive, educational, and digitally integrated approach.
Call to Action for Policymakers and Global Health Stakeholders:
- Mandate Digital Health Integration in UHC: As Kenya rolls out the Social Health Authority (SHA), digital health literacy tools must be integrated into the primary care package. Reimbursing clinics that utilize AI triage systems will incentivize the adoption of these life-saving tools.
- Invest in Localized AI Infrastructure: Governments and private investors must fund the development of open-source clinical datasets reflecting African phenotypes and linguistics. This will prevent algorithmic bias and ensure AI tools are accurate for the populations they serve.
- Empower Community Health Promoters (CHPs): Technology should augment human touch. Equipping Kenya’s network of CHPs with AI-enabled diagnostic tablets transforms them from mere data collectors into empowered, mobile diagnostic hubs capable of educating households on the spot.
- Radical Patient Education: We must treat health illiteracy as aggressively as we treat a viral outbreak. Public schools must integrate comprehensive health literacy into the national curriculum, teaching children the basic tenets of NCD prevention, mental health awareness, and reproductive health.
“When an old man dies, a library is burned with him.”Contextual Analysis: Historically, indigenous knowledge and community health wisdom were passed down orally by elders. In the modern era, as we face new, complex diseases, the new “library” must be a digital one. By feeding AI with localized data and making it accessible to every mother and father, we ensure that the library of health knowledge is never burned, but distributed to all.
9. Conclusion
The tragedy of healthcare in Sub-Saharan Africa is not merely that people suffer from diseases; it is that they suffer from diseases that are eminently preventable and treatable. Healthcare illiteracy forms an invisible, suffocating barrier between life-saving medical science and the communities that desperately need it. As we have seen in the Kenyan context, ignorance fuels a cascade of systemic failures—from late-stage cancer diagnoses to devastatingly high maternal mortality rates.
However, the dawn of the Digital Renaissance offers unprecedented hope. Through the strategic, culturally competent deployment of Artificial Intelligence, mHealth platforms, and digital diagnostic tools, organizations like Jacaranda Health and Ilara Health are proving that it is possible to democratize medical knowledge at scale. By transforming every basic mobile phone into a trusted health companion and triage center, we can dismantle the epidemic of ignorance. To reiterate the profound wisdom of the African proverb: “Knowledge is a garden. If it isn’t cultivated, you can’t harvest it.” It is time for Africa to aggressively cultivate health literacy through the power of AI, ensuring a harvest of longevity, equity, and health for generations to come.
References
Asava, S. K. (2025). If we get education and healthcare wrong, we die twice – poor and stupid. Citizen Digital. Retrieved from Citizen Digital Archives.
Kenya National Bureau of Statistics. (2022). Kenya Demographic and Health Survey (KDHS) 2022. Government of Kenya.
Ministry of Health, Republic of Kenya. (2024). Every Suicide Is A Preventable Tragedy, A Need For An Integrated Care Model In Kenya. Mental Health Policy Brief.
OECD. (2025). Health at a Glance 2025: Avoidable mortality (preventable and treatable). OECD Publishing.
Onyango, J., & Onyango, M. (2022). Assessment of Factors Influencing Non-Communicable Diseases Literacy Levels in Vihiga County–A Qualitative Cross-Sectional Study. European Journal of Environment and Public Health.
Rockefeller Foundation. (2024). AI Meets Motherhood to Bridge the Information Gap in Africa. Grantee Impact Stories.
Connecting Africa. (2024). Ilara Health aims to improve quality of care in Kenya. Innovation Hub.
The HealthTech. (2024). Healthtech Startups in Kenya. Ventures Report.
Wabwire, E., et al. (2024). Fear, faith and finances: health literacy experiences of English and Swahili speaking women newly diagnosed with breast and cervical cancer. PMC Archives.
World Health Organization. (2025). Health literacy – Fact Sheets. WHO Publishing.
Zheng, M., et al. (2021). Association between health literacy and mortality: a systematic review and meta-analysis. PMC Archives.

{kind=link}
Leave Your Comment